- Visibility 78 Views
- Downloads 19 Downloads
- DOI 10.18231/j.ijpca.2021.003
-
CrossMark

A review: Pathophysiology, diagnosis and management of multiple sclerosis
Introduction
Multiple sclerosis is an auto immune disorder that affectscentral nervous system and it leads to severe physical and cognitive incapacitation as well as neurological problems in young adults. However MS is somewhat influenced by B cells through a variety of mechanisms, including ectopic lymphoid follicles in the CNS, present antigen , production of cytokine and production of antibiotics. Multiple sclerosis is considered the most common cause of neurological disability while inflammatory lesions associated with MS may affect a large range of systems and cause a variety of neurological symptoms.[1], [2]
Multiple sclerosis presents between 20 and 40 years of age and the women are more susceptible than men. The exact pathophysiology of multiple sclerosis in not known but it seems to be autoimmune in nature.[3]
Types of Multiple Sclerosis[4], [5], [6]
Multiple sclerosis is extremely variable with symptoms that may be appear, disappear or sometimes worsen over time and it is possible and to classify people according to the course of their disease.
Relapsing remitting multiple sclerosis
Secondary progressive multiple sclerosis
Primary progressive multiple sclerosis
Progressive relapsing multiple sclerosis
The treatment strategy for multiple sclerosis is broadly based on disease – modifying drugs such as interferon – β and glatiramer acetate. Multifocal zones of inflammation due to T- lymphocyte and macrophage infiltrations and are the primary causes of myelin sheath destruction that result in the formation of CNS plaques.
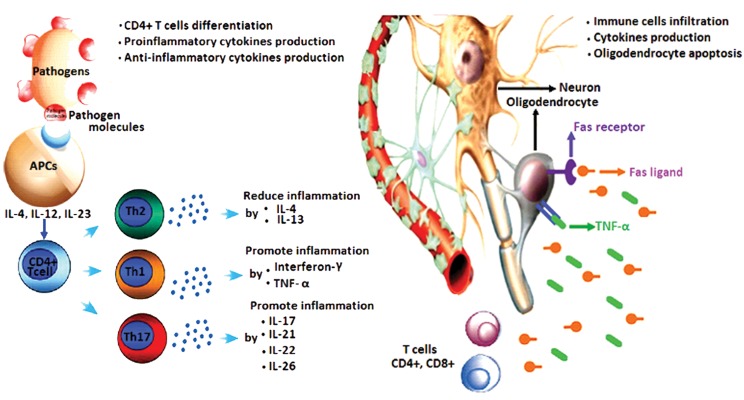
Pathogenesis of Multiple Sclerosis
Multiple sclerosis shows a variety of neurological symptoms that spread in different parts of the CNS. It may occur alone or combined. These symptoms are quite vary from patient to patient but it may involve sensory disturbance, dysfunction of bladder, vision loss limb weakness, fatigue and troubles in bowel. Typically the disease starts with the sudden onset of neurological deficits.[7], [8]
Only small percentage of patients feel a gradually progressive clinical course from the onset of the disease such as clinical course refers to the principal progressive from of MS. Therefore the steady progression of symptoms associated with primary progressive MS leads to disability from the beginning.[9], [10]
Diagnosis Approaches
Basically the diagnosis of multiple sclerosis is based on the demonstration of MS- typical CNS lesions disseminated in space and time which based upon clinical findings alone or it a combination of clinical and MRI approach. It’s also being diagnosed with the demonstration of neurological sign and symptoms.[10], [11], [12]
|
Primary symptoms |
More common symptoms |
Dizziness, emotional impairment, vision problems and walking difficulty |
|
Less common symptoms |
Hearing, Headache, breathing and Speech problems and swallowing etc. |
|
|
Secondary symptoms |
Urinary tract infections |
|
|
Tertiary symptoms |
Depression, Psychological and social complications. |
|
Nowadays the diagnosis of MS based on the result of MRI examination. For MRI examination a contrast agent like gadolinium used to highlight active plaques, MRI allows detecting plaques that are ongoing to destruction of the BBB. Apart of this diagnosis tools various potentials test including visual, brain stem auditory and somatosensory, these furnished the information about demyelization in the optic nerve and CNS. In addition, CSF analysis for myelin basic protein and immunoglobulin gamma (Ig G) determination and blood sample analysis for detection of vitamin deficiencies may be helpful.[13], [14]
Management of Multiple Sclerosis
In previous studies we know that there is no current treatment of multiple sclerosis but Therapeutic management may be useful. Therapeutic management can be dividing into relapse treatment, Symptomatic treatment and disease- modifying treatment. In relapse treatment the Methylprednisolone at dose of 1 g/day or 500 mg/day for 305 days with or without oral tapering. Alternatively the treatment continues with equal dose via oral administration.
In disease- modifying treatment, potentially ameliorate the disease course are studied and in case the clinical course is dominated by relapses as for the clinically isolated syndrome RRMS and occasionally SPMS.
The basic therapeutics deals with immunomodulators like IFN β and glatiramer acetate are used as first line therapeutics which help in reducing the relapse rate and do not cause any severe side effect. Teriflunomide and fingolimod are also used as basic therapeutics.
Basic therapeutics Apart from above treatment some therapies like Escalation therapy and Symptomatic treatment etc. are also available which more beneficial in the treatment of multiple sclerosis.[15], [16]
Conclusion
The actual cause of multiple sclerosis is unknown. Various factors influences play an important role in the pathogenesis of this disease. Several drugs having therapeutic effect anti inflammatory drugs, immunomodulators in multiple sclerosis have been studied. In present research, current treatment is not available but beside drug therapies like ADSCs which gives the idea of cell transplantation. This idea may provide a novel strategy for the treatment of neurological disease.
Source of Funding
None.
Conflict of Interest
The authors declare that there is no conflict of interest.
References
- C Bjartmar, JR Wujek, BD Trapp. Axonal loss in the pathology of MS: consequences for understanding the progressive phase of the disease. J Neurol Sci 2003. [Google Scholar] [Crossref]
- T Jersild. Penicillin in Scarlet Fever. BMJ 1948. [Google Scholar] [Crossref]
- BD Trapp, KA Nave. Multiple Sclerosis: An Immune or Neurodegenerative Disorder?. Annu Rev Neurosci 2008. [Google Scholar] [Crossref]
- A Alonso, MA Hermain. Temporal trends in the incidence of multiple sclerosis: a systemic review. Neurology 20008. [Google Scholar]
- R Gandhi, A Laroni, HL Weiner. Role of the innate immune system in the pathogenesis of multiple sclerosis. J Neuroimmunol 2010. [Google Scholar] [Crossref]
- NG Torkildsen, SA Lie, HL Nyland. Survival and cause of death in multi sclerosis. Neurol Mult Scaler 2008. [Google Scholar]
- EG Celius, C Smestad. Change in sex ratio, disease course and age at diagnosis in Oslo MS patients through seven decades. Acta Neurol Scand 2009. [Google Scholar] [Crossref]
- IF Charo, RM Ransohoff. The Many Roles of Chemokines and Chemokine Receptors in Inflammation. N Engl J Med 2006. [Google Scholar] [Crossref]
- FD Lublin, SC Reingold. Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurology 1996. [Google Scholar]
- AJ Coles, A Cox, E Page, J Jones, SA Trip, J Deans. The window of therapeutic opportunity in multiple sclerosis. J Neurol 2006. [Google Scholar] [Crossref]
- A Feinstein. . The clinical neuropsychiatry of multiple sclerosis 2007. [Google Scholar]
- RA Marrie, R Rudick, R Horwitz, G Cutter, T Tyry, D Campagnolo. Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology 2010. [Google Scholar] [Crossref]
- DH Mahad, BD Trapp, H Lassmann. Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol 2015. [Google Scholar] [Crossref]
- R Milo, A Miller. Revised diagnostic criteria of multiple sclerosis. Autoimmun Rev 2014. [Google Scholar] [Crossref]
- B Ferguson, MK Matyszak, MM Esiri, VH Perry. Axonal damage in acute multiple sclerosis lesions. Brain 1997. [Google Scholar]
- F Khan, L Turner, T Kilpatrick. Multidisciplinary rehabilitation for adults with multiple sclerosis. J Neural Neurosurg Psychiatry 2008. [Google Scholar]